THE TITLE IS YOUR RESEARCH
The Title Is the Research: Why Getting It Right Is Not Optional for PG and PhD Scholars in Ayurveda
| Dr. Aakash Kembhavi MD (Ayu-Shalya), PGDMLS, MS (Counseling & Psychotherapy) |
Every year, thousands of postgraduate and doctoral scholars in Ayurveda sit before their synopsis committees with weeks, sometimes months, of preparation behind them. And yet, the single most visible element of that preparation — the research title — remains, in a surprising number of cases, embarrassingly vague, clinically unanchored, and scientifically unjustifiable.
This is not a peripheral problem. The title of a research synopsis is not a label. It is a condensed research question. It is a contract with the reader about what will be studied, in whom, through what lens, and toward what end. When the title fails, the entire architecture of the study collapses — even before a single patient is enrolled.
This article is an attempt to address that failure systematically. I will walk you through the PICO framework, explain why it is not optional, unpack the role of critical literature search and relevance analysis in title construction, and demonstrate each component with Ayurveda-specific examples: the wrong title first, followed by what it should have been and why.
Why the Title Matters More Than Scholars Realise
Before we enter the framework, let us understand the stakes.
The title of your synopsis does several things simultaneously:
It defines the scope of your study. A poorly framed title will either commit you to doing far more than is feasible within an MD or PhD programme, or will produce research so narrow and trivial that it fails to add any meaningful knowledge.
It determines the kind of research design you must use. A title that implies comparison demands a comparative study. A title that implies therapeutic efficacy demands a clinical trial. When scholars write titles that are ambiguous about what they intend to compare, in whom, and against what control, they simultaneously make it impossible for the ethics committee, the guide, and the examiner to evaluate the proposal on sound methodological grounds.
It signals your understanding of the literature. An informed scholar does not propose a title for a study that has already been done — or worse, one that cannot even be done given the clinical and ethical constraints of Ayurvedic practice. The title is your first public statement of your scholarly calibre.
It protects you legally and ethically. An imprecise title that promises outcomes your study cannot measure — or implies causation where you are only observing correlation — is a source of post-submission grief. Synopsis committees have every right to reject a title that is not scientifically defensible, and increasingly, they are exercising that right.
The PICO Framework: What It Is and Why It Is Non-Negotiable
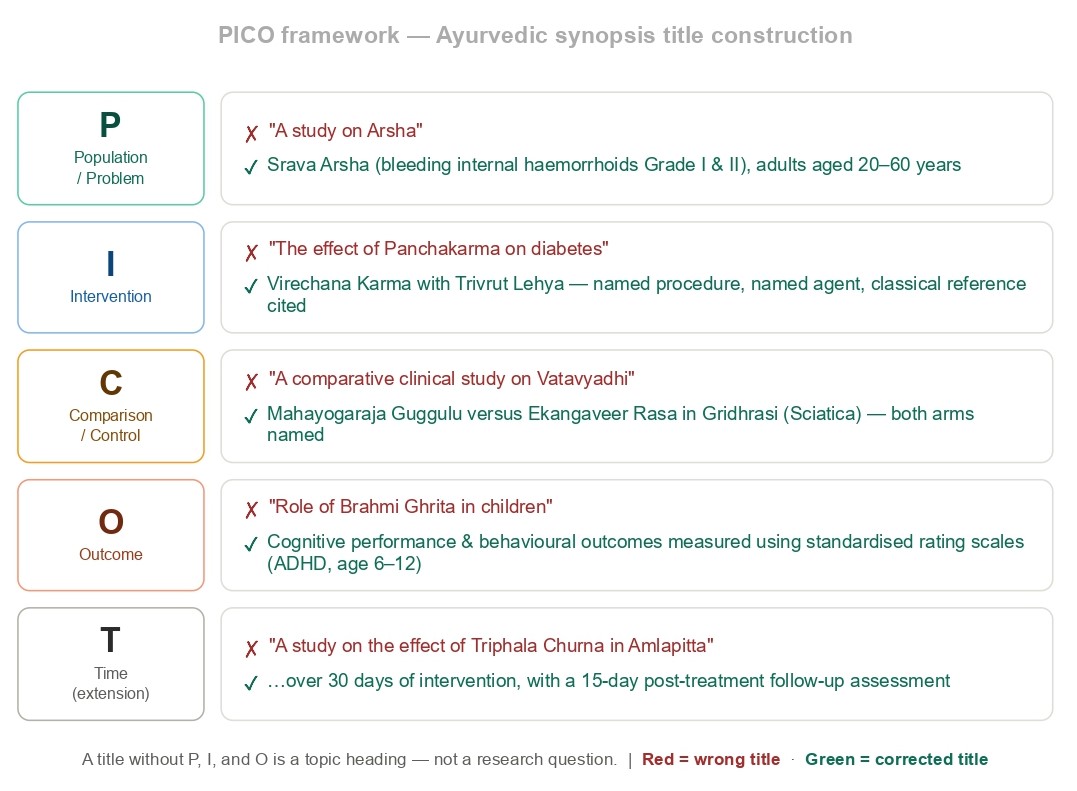
PICO is a structured tool for framing a researchable clinical question. The acronym stands for:
- P — Population (or Problem): Who are you studying? What is the defined group?
- I — Intervention: What are you doing to them, or what are they exposed to?
- C — Comparison (or Control): What is the intervention being compared to, if anything?
- O — Outcome: What are you measuring? How will you know your intervention worked, or didn’t?
In some contexts, the framework is extended to PICOT (adding Time) or PICOS (adding Study design), but for the purposes of a PG or PhD synopsis in Ayurveda, ensuring that all four core components are either explicitly present or clearly implied in the title is the minimum acceptable standard.
Guides and scholars often object that “this is an evidence-based medicine (EBM) tool imported from Western medicine and does not fit Ayurveda.” This objection, while understandable, is not valid. PICO is not a philosophical framework. It is a precision tool. The question “What does Ashwagandha do for fatigue in anaemic women?” is a PICO question whether it is asked in a biomedical or Ayurvedic research context. The classical Ayurvedic tradition itself — from Charaka’s systematic inquiry into Satmya, to Sushruta’s documentation of surgical outcomes, to the Rasashastra texts’ meticulous mapping of preparation methods to therapeutic results — demands this same precision. PICO simply gives it a modern vocabulary.
Let me be direct: a title that does not answer at least implicitly to P, I, and O is not a research title. It is a topic heading. And a topic heading is not eligible to become a research study.
Breaking Down PICO with Ayurveda Examples
Component 1: P — Population (or Problem)
What it demands: The population must be defined by age group, gender (if relevant), diagnosis (both in Ayurvedic and/or contemporary clinical terms), stage or severity of the condition, and any relevant exclusion criteria implied by the context.
Wrong title:
“A study on Arsha”
This tells us nothing. Arsha is a broad category encompassing multiple types — Sahaja and Janmottara, Shushka and Srava, internal and prolapsed, complicated and uncomplicated. Is this a study on first-degree haemorrhoids? Second-degree bleeding piles in adults? Arsha with concomitant Grahani? Without specifying the population, you cannot design an ethical, reproducible study.
Corrected title:
“A clinical study to evaluate the efficacy of Kasisadi Taila Pichu in the management of Srava Arsha (bleeding internal haemorrhoids Grade I and II) in adult patients between 20–60 years of age”
Now we know who is being studied, at what stage of the condition, and in what age group. The clinical and Ayurvedic diagnosis run parallel. The study can be reproduced.
Component 2: I — Intervention
What it demands: The intervention must be named precisely — including the formulation name, route of administration, dosage (where applicable), duration of administration, and the classical reference or pharmacopoeial source for the preparation.
Wrong title:
“The effect of Panchakarma on diabetes”
“Panchakarma” is not one intervention. It is a system comprising five major procedures, each with its own preparatory (Purvakarma) protocols, each applicable based on individual Prakriti, Vikara, Kala, and Bala. “Diabetes” is not a clinical category in Ayurveda. This title is not even vague — it is incoherent. No ethics committee can approve a study it cannot evaluate.
Corrected title:
“Efficacy of Virechana Karma with Trivrut Lehya in the management of Prameha (Type 2 Diabetes Mellitus) — a randomised controlled pilot study”
Now the procedure is named (Virechana), the therapeutic agent is named (Trivrut Lehya), the condition is given both Ayurvedic and contemporary equivalent labels, and the study design is declared. A reader knows immediately what this study will do and what it will not do.
Component 3: C — Comparison (Control)
What it demands: For clinical trials, the comparison group must be specified. Are you comparing an Ayurvedic intervention to a placebo, to standard biomedical care, to another Ayurvedic formulation, or to a no-treatment control? For observational studies, comparison may be implicit (before versus after), but this too must be stated or clearly implied.
This is the component most frequently missing or ambiguous in Ayurvedic PG titles. Scholars either omit the control entirely, or they use the phrase “comparative study” in the title without telling the reader what is being compared to what.
Wrong title:
“A comparative clinical study on Vatavyadhi”
Comparative with what? Comparing which interventions? In which population? This title is uninformative to the point of being meaningless. “Comparative” has become a cargo-cult word in Ayurvedic synopsis writing — it is used because it sounds scientific, not because it commits the researcher to anything.
Corrected title:
“A randomised comparative clinical study to evaluate the efficacy of Mahayogaraja Guggulu versus Ekangaveer Rasa in the management of Gridhrasi (Sciatica) with special reference to pain and functional disability”
Now the comparison is explicit — drug A versus drug B. The condition is named in both classical and contemporary terms. The outcomes are stated. A reader can immediately understand the research design implied by this title.
Component 4: O — Outcome
What it demands: The outcome(s) must be measurable, predefined, and appropriate to the condition being studied. The best titles either name the outcome directly or make it strongly implied through the clinical terminology used. Outcome measures in Ayurvedic research can include validated symptom scales, classical Lakshana-based scoring, laboratory parameters, or a combination of both.
The absence of a clearly stated outcome is the reason so many Ayurvedic clinical studies end up measuring something that was not the real purpose of the intervention. When the title does not specify what is being measured, it is because the researcher has not yet decided — and that is a protocol problem masquerading as a title problem.
Wrong title:
“A clinical study on the role of Brahmi Ghrita in children”
“Role” is not an outcome. “In children” is not a population. This title commits to nothing and therefore cannot be evaluated. What aspect of Brahmi Ghrita is being studied? Memory enhancement? Attention deficits? Specific age group within children? Diagnosed with what — Unmada? ADHD? Does “role” mean efficacy, safety, tolerability, or all three?
Corrected title:
“A clinical evaluation of Brahmi Ghrita in the management of Medo-Majja Gata Vata presenting as Attention Deficit Hyperactivity Disorder (ADHD) in children aged 6–12 years: assessment of cognitive performance and behavioural outcomes using standardised rating scales”
Now the drug, the population, the condition in both Ayurvedic and contemporary terminology, and the outcome measures are all present. This is a fundable, approvable, reviewable research question.
The PICOT Extension: Adding Time
In longitudinal studies, the element of Time (T) becomes critical. How long will the intervention run? At what point will outcomes be measured? Is there a follow-up period?
Wrong title:
“A study on the effect of Triphala Churna in the management of Amlapitta”
Corrected title (with T):
“A clinical study to evaluate the efficacy of Triphala Churna in the management of Amlapitta (Gastro-Oesophageal Reflux Disease) over 30 days, with a 15-day follow-up assessment”
The addition of time transforms a vague proposal into a structured protocol. It tells the reader — and the ethics committee — exactly how long the study runs, when outcomes are captured, and whether the intervention’s effects are sustainable.
The Critical Literature Search: The Foundation You Cannot Skip
No title should ever be written before the researcher has conducted — and genuinely understood — a thorough review of the existing literature. This is not bureaucratic formality. It is intellectual due diligence. Here is why, and how much is expected.
Why the Literature Search Is Constitutive of the Title
The title of your synopsis is a claim that this research is needed. It is an implicit argument that the question you are asking has not been adequately answered. Without a literature search, you are making that claim in the dark. And guides, co-guides, and examiners who are familiar with the existing literature will know it.
A proper literature search performs three functions:
First, it establishes the evidence gap. If ten well-designed RCTs have already evaluated Kanchanar Guggulu in Hypothyroidism and shown consistent results, proposing yet another open-label clinical study on the same intervention in the same condition is not research — it is repetition. Your title must be positioned against what is already known.
Second, it identifies the right outcome measures. The literature will tell you what has been measured before, what scales have been validated, and what gaps remain in outcome assessment. A scholar who proposes a study on Cognitive Performance after reading that previous studies used only informal memory tasks will immediately know to specify a validated tool like RAVLT or MMSE in their title.
Third, it prevents methodological and ethical errors. If the existing literature has documented significant adverse effects of a compound at certain doses, a title that does not acknowledge this safety context will raise immediate red flags at the ethics committee.
How Much Literature Should Be Reviewed?
For a PG synopsis, a minimum of 30–50 references drawn from peer-reviewed Ayurvedic, biomedical, and pharmacological literature is expected — not for cosmetic purposes, but to demonstrate real familiarity with the field. For a PhD synopsis, the bar rises significantly: 80–120 references is the starting point, with a clear systematic analysis of study designs, outcome measures, methodological limitations, and consensus gaps in prior research.
Sources should include: classical Ayurvedic texts (Charaka, Sushruta, Ashtanga Hridayam, Madhava Nidana, relevant Nighantus); AYUSH-funded research databases (DHARA, CCRAS repository); indexed Ayurvedic journals (AYU, Journal of Ethnopharmacology, Journal of Ayurveda and Integrative Medicine); PubMed, Scopus, and Web of Science for pharmacological and clinical data; and Cochrane reviews where systematic evidence has been synthesized.
The literature search should culminate not in a bibliography appended to the synopsis, but in a narrative understanding of what is known, what is disputed, what is missing, and why your proposed study addresses a genuine knowledge gap.
The Relevance Test: Does Your Title Pass?
Even a well-structured PICO title can fail the relevance test. Before finalising your title, ask yourself:
Is this condition prevalent enough to justify a study? A study on a condition seen in fewer than five patients per year at your institution will fail at the patient recruitment stage regardless of how elegant the title is.
Is this intervention practically administrable? If the classical formulation requires ingredients that are Schedule I restricted or commercially unavailable, your title proposes a study you cannot conduct.
Does the outcome measure capture what the intervention is actually expected to do? If you are studying Shirodhara for Stress-related Insomnia, measuring only ESG (electroencephalography) without capturing subjective sleep quality and psychological parameters fails to address the most clinically relevant dimensions of the intervention.
Is the title ethically defensible? Can the study be conducted without withholding standard of care? Can informed consent be meaningfully obtained? Does the study timeline align with the natural course of the disease?
A title that fails any of these questions must be revised — not defended, not explained away, but revised.
The Open-Label Problem: A Systemic Epistemological Failure in Ayurvedic Research Titles
If there is one phrase that has done more damage to the credibility of Ayurvedic clinical research than any other, it is the phrase “open-label randomised controlled trial” — used casually, incorrectly, and with alarming frequency in PG synopsis titles across institutions affiliated with every major Ayurvedic university in the country.
Let us be precise about what these terms mean, what they demand, and why using them loosely is not merely a semantic error but an epistemological one — a failure of the scholar’s fundamental understanding of knowledge, evidence, and the conditions under which a claim about therapeutic efficacy can be made.
What an Open-Label Trial Actually Means
An open-label trial is one in which both the researcher and the participant are aware of which treatment is being administered. There is no blinding — not of the patient, not of the clinician, not of the assessor. This design is legitimate in specific contexts: early-phase safety studies, dose-finding studies, pragmatic effectiveness studies in real-world conditions, or studies of interventions where blinding is structurally impossible (such as surgical procedures or complex Panchakarma protocols).
The key epistemological implication of an open-label design is this: it is maximally susceptible to bias. When a patient knows she is receiving an Ayurvedic intervention, her expectation of benefit is activated. When a clinician knows which group a patient is in, his assessment of symptom improvement is influenced — consciously or otherwise. When the assessor is the treating physician, the measurement and the treatment are no longer independent. These are not theoretical concerns. They are the mechanisms by which open-label studies systematically overestimate treatment effects, and the literature on this is unambiguous.
This does not make open-label studies worthless. It makes them appropriate for certain questions and inappropriate for others. Specifically, an open-label design cannot support efficacy claims. It can support feasibility claims, safety claims, and preliminary signal detection. The moment a scholar uses an open-label design and then claims to have “proven” that Drug X is “effective” in Condition Y, the study has crossed an epistemological boundary it is not equipped to cross.
What a Randomised Controlled Trial Actually Demands
A Randomised Controlled Trial (RCT) is a study design with four non-negotiable structural features:
Randomisation — participants are allocated to treatment groups by a process that is genuinely random (computer-generated random sequence, sealed envelope allocation from a centralised system, or similar), not by convenience, not by the physician’s clinical judgment, and not by alternating allocation (ABAB), which is quasi-randomisation and categorically different.
A Control group — there is a comparison group that receives either a placebo, standard of care, or an active comparator. A study with only one treatment arm has no control. It is a before-after study, not a controlled trial.
Allocation concealment — the allocation sequence must be concealed from the individuals responsible for enrolling participants, so that foreknowledge of the next assignment cannot influence enrolment decisions. Without allocation concealment, even genuine randomisation can be subverted.
A pre-specified primary outcome — the outcome being used to evaluate the intervention must be decided before the study begins, not after looking at what improved the most. Post-hoc outcome selection is one of the most common and most invisible forms of research misconduct.
When scholars append the label “RCT” to a study that has sequential allocation, no allocation concealment, a single treatment arm evaluated before and after, and outcomes chosen because they showed significance — they are not conducting an RCT. They are conducting an uncontrolled before-after study and misrepresenting it with a label that implies a level of methodological rigour the study does not possess.
The Specific Mutations Found in Ayurvedic Synopsis Titles
Several hybridised, internally contradictory phrases have become standard in Ayurvedic synopsis writing. Each of them represents a distinct category of epistemological error.
“Open-label randomised controlled trial”
This phrase is the most common and the most confused. An open-label study can be randomised. It can have a control group. But when Ayurvedic scholars write this phrase, they almost invariably mean: patients were assigned to two groups (often sequentially or by odd-even numbering), both groups knew which treatment they were receiving, the treating physician administered and assessed the treatment, and the study had no placebo arm. What they have described is an open-label comparative study at best — and that is a legitimate design, but it carries entirely different inferential weight than a blinded RCT. The confusion between the two is not trivial. It is the difference between a study that can support a moderate efficacy claim and one that can support a claim about superiority with confidence.
“Randomised double-blind placebo-controlled trial” in a context where blinding is impossible
Scholars sometimes adopt this language because it sounds like the gold standard — which it is, in biomedical research. But proposing a double-blind placebo-controlled trial for Panchakarma, Agnikarma, Ksharakarma, or any complex multi-modal Ayurvedic intervention is methodologically incoherent. You cannot blind a patient to the fact that they are receiving Basti or Virechana. You cannot create a placebo for Agnikarma that is ethically administrable. Claiming a double-blind design for these interventions is not aspirational — it is false. The title promises what the study structurally cannot deliver.
“Single-group open-label clinical trial”
This phrase attempts to reconcile the desire for “trial” language with the absence of a control group. But a trial without a control is not a trial in any epistemologically meaningful sense. It is an observational study with an intervention. The word “trial” implies that a hypothesis is being tested under conditions that allow causal inference. Without a control group, you are observing what happens to patients who receive an intervention over time. Many things happen to patients over time — natural disease remission, seasonal variation, regression to the mean, concurrent lifestyle changes, and the Hawthorne effect. An uncontrolled study cannot distinguish between these and the effect of the intervention.
“Comparative randomised study” without specifying what is being compared
As discussed in the PICO section, “comparative” without naming both arms is meaningless. But the deeper error here is that scholars sometimes describe a study as “randomised” when what they mean is that they alternated patients between two groups — Group A, Group B, Group A, Group B — in a fixed sequence. This is not randomisation. This is allocation by sequence. The difference matters because sequential allocation allows selection bias: a physician who knows the next patient will go into Group B may (consciously or not) enrol a different type of patient than if the allocation were genuinely unpredictable.
Why This Is an Epistemological Failure, Not Just a Labelling Error
The errors described above are not merely technical. They reflect a deeper misunderstanding about the relationship between research design and the claims it can support.
Epistemology — the study of knowledge, its sources, and its limits — tells us that the strength of a claim must be matched to the strength of the evidence that supports it. An open-label before-after study generates a hypothesis. A well-conducted RCT tests that hypothesis under conditions designed to eliminate alternative explanations. These are not interchangeable. They produce different kinds of knowledge, and they warrant different kinds of claims.
When a scholar conducts an open-label convenience-sample study and titles it as an RCT, one of two things is true: either the scholar does not understand what an RCT requires (a knowledge failure), or the scholar understands but uses the label anyway for its rhetorical power (an integrity failure). Both are serious. The first is a failure of training. The second is a failure of scholarly ethics.
The broader consequence is this: when Ayurvedic research is built systematically on mislabelled designs, the field’s evidence base becomes inflated. Studies appear more rigorous than they are. Meta-analyses that pool these studies produce findings that overestimate treatment effects. Regulatory submissions based on this evidence are vulnerable to challenge. Patients and physicians who rely on these findings to make treatment decisions are being misled — not by malice, but by a systemic failure to teach scholars what their study designs actually mean.
This is not an argument against Ayurvedic research. It is an argument for doing it honestly.
The Cascading Comparator Problem: When a Flawed Study Becomes a Standard
There is a second, equally serious error embedded in the comparative design of most Ayurvedic clinical studies, and it deserves its own examination because it is both more subtle and more structurally damaging than the open-label labelling confusion.
It works like this.
A PG scholar at Institution A conducts an open-label, 30-patient study comparing Formulation X to no treatment in Condition Y. The results favour Formulation X. The study is submitted, accepted, and published — often in a non-indexed or minimally-indexed Ayurvedic journal with no peer review of methodology. Two years later, a scholar at Institution B proposes a synopsis in which Formulation Z is compared against Formulation X — now cited as the “standard comparator” or “established drug of reference.” The guide approves it. The ethics committee approves it. The study is conducted with another 30 patients, open-label, no blinding, with the treating physician as assessor. Formulation Z performs comparably to Formulation X. The conclusion reads: “Formulation Z is equally efficacious to the established Ayurvedic standard Formulation X, with added benefits of…” And so the cycle continues.
What has actually been established? Nothing. The comparator was never validated. The original study had no control arm, no blinding, a sample size adequate only to detect the most dramatic of effects, and a design that systematically overestimated the response. Comparing a new drug to that comparator is not comparative research. It is the comparison of two unknowns, one of which has been granted the false status of a known.
This is not an isolated pattern. It is the dominant architecture of comparative Ayurvedic clinical research in India today.
What Makes a Legitimate Comparator
A legitimate comparator in a clinical study must satisfy at least one of the following conditions:
It is a drug or intervention whose efficacy has been established through adequately powered, methodologically sound trials — ideally with replication across independent centres, or through a systematic review or meta-analysis that pools evidence from multiple studies of acceptable quality.
It is the current standard of care as defined by a recognised clinical guideline — national or international — against which the experimental intervention is being tested for non-inferiority, equivalence, or superiority.
It is a validated active control whose mechanism, dosage, and outcome profile are well characterised in the existing literature, making it possible to interpret what a “comparable” result with the new intervention actually means.
An Ayurvedic formulation evaluated in a single open-label PG study with 20 or 30 patients, no control group, and an outcome assessment conducted by the treating physician meets none of these conditions. It is not a standard. It is a preliminary observation that was never adequately tested and should never have been promoted to the status of a reference treatment.
Why Sample Size Is Not a Minor Technical Detail
The casual acceptance of 20–30 patient studies as sufficient evidence for comparative reference is a symptom of a deeper failure to understand statistical inference. A study that is not adequately powered does not merely produce uncertain results — it produces systematically distorted ones.
When a study is underpowered, it is unlikely to detect a true effect if one exists (low sensitivity). But the studies that do show significant results in small samples are disproportionately those that caught an extreme random fluctuation — not a real treatment effect. This is the winner’s curse in clinical research: the studies that get published from small samples tend to be the ones with the largest effect sizes, because those are the ones that crossed the significance threshold. They are the least likely to be representative of the true effect, and they are the most likely to fail replication.
When the next generation of scholars takes these inflated effect estimates as the benchmark for their comparator, they are designing studies to beat a target that was never real. The entire comparative edifice is built on a statistical artefact.
The minimum sample size for a comparative clinical study in Ayurveda must be calculated a priori — before the study begins — based on the expected effect size, the chosen level of statistical significance (alpha), the desired power (1-beta, conventionally 80% or 90%), and the variability of the primary outcome measure. This calculation must be grounded in data from adequately conducted prior studies or in conservative estimates where such data do not exist. A sample size of 30 per group that has not been derived through this process is not a clinical decision. It is a convention masquerading as a calculation.
The Epistemological Consequence: A Self-Referential Evidence Loop
What the cascading comparator pattern creates, at the level of the field as a whole, is a self-referential evidence loop. Ayurvedic PG research increasingly cites Ayurvedic PG research as its evidence base, with no external validation, no independent replication, and no methodological audit of the studies being cited. The loop is closed. External scrutiny cannot enter because the field has built its own internal citation ecosystem in which internally generated, methodologically weak studies validate each other in perpetuity.
This is not unique to Ayurveda. It is a known failure mode in any research tradition that lacks robust peer review, independent replication requirements, and methodological gatekeeping. But it is particularly acute in Ayurveda because the tradition’s epistemological richness — its sophisticated theories of pramana, its layered understanding of cause and effect in biological systems — is entirely compatible with rigorous research design. The failure is not inherent to the knowledge system. It is a failure of the institutions that produce researchers, the journals that publish without methodological scrutiny, and the guides who approve comparators without asking what evidence established them as standard.
What Should Appear in the Title and Protocol Instead
If the only available comparator is a previously studied Ayurvedic formulation from a methodologically limited study, the scholar has two honest options.
The first is to acknowledge this explicitly in the synopsis and design the study accordingly — not as a comparative efficacy trial, but as a pilot comparative study generating preliminary data, with a clearly stated limitation that the comparator itself has not been validated by adequately powered research. The title should reflect this: “a pilot comparative study” or “a preliminary comparative evaluation,” not a “randomised controlled trial establishing the efficacy of Formulation Z against the established standard Formulation X.”
The second, more ambitious and more scientifically valuable option is to use a placebo control or a biomedical standard of care as the comparator — where ethically feasible — and to test both the experimental Ayurvedic formulation and the existing Ayurvedic reference drug in a three-arm design. This immediately elevates the study’s inferential value and generates data that can contribute to genuine comparative knowledge rather than circular self-reference.
What scholars must stop writing in their titles is the phrase “as compared to standard drug” or “versus established Ayurvedic formulation” when the “standard” in question is a single low-powered open-label study from a PG dissertation. The title implies a knowledge claim the evidence does not support. That implication, repeated across thousands of synopses, compounds into a systematic misrepresentation of what Ayurvedic clinical science actually knows.
What the Title Should Declare — and What Scholars Should Stop Writing
If your study has two treatment arms, sequential allocation, no placebo, no blinding, and you are the treating physician and the assessor: call it an open-label comparative clinical study. That is what it is. It is a legitimate design with real utility. Own it.
If your study has one treatment group evaluated before and after intervention: call it a single-arm prospective observational study or a before-after interventional study. Do not call it a trial.
If your study genuinely has computer-generated randomisation, a control arm, allocation concealment, and independent outcome assessment: then, and only then, call it a randomised controlled trial — and open-label or blinded, as the case may actually be.
The title of your synopsis is not the place for aspirational design claims. It is the place for accurate ones.
A Note on Language and Terminology in the Title
Ayurvedic PG and PhD titles must navigate a dual terminological system: classical Ayurvedic nomenclature and contemporary biomedical language. Both have a role in the title, but they must be used with precision.
Do not conflate classical entities with contemporary diagnoses. Pandu and Iron Deficiency Anaemia are not the same condition. They can be correlated, mapped, and studied in parallel, but a title that says “Pandu (Iron Deficiency Anaemia)” is implicitly claiming an equivalence that requires justification. Consider instead: “Pandu with reference to Iron Deficiency Anaemia” or “Pandu as a clinical correlate of Iron Deficiency Anaemia.”
Do not use Sanskrit terms without a contemporary equivalent in a biomedical research context. If your synopsis is going to an ICMR ethics committee or a biomedical journal, a title that reads only in classical terms will face immediate clarification requests. Dual nomenclature is not a compromise — it is accurate representation of your research context.
Keep the title to one sentence, ideally under 25 words in the main clause. Every additional clause is a potential source of scope ambiguity. If you cannot express your research question in a single clean sentence, your research question is not yet clear enough to become a study.
The Institutional Failure: When the System Certifies What It Should Correct
Everything described in this article — the PICO-less title, the mislabelled study design, the cascading comparator built on a methodologically bankrupt predecessor — would be containable if the systems designed to catch these errors were functioning. They are not.
The most uncomfortable truth about the state of Ayurvedic postgraduate and doctoral research is not that individual scholars make these mistakes. Scholars at all levels of any discipline make mistakes. The purpose of the institutional architecture surrounding research — the guide, the synopsis committee, the departmental review, the university registration process, the dissertation examiner, the viva voce panel — is precisely to catch those mistakes before they become credentialed claims about therapeutic efficacy. In Ayurveda, that architecture has, in a significant proportion of cases, ceased to perform that function.
Synopses Are Being Registered With These Errors Intact
Across institutions affiliated to RGUHS, Gujarat Ayurved University, MUHS, Rajasthan Ayurved University, and the majority of state Ayurvedic universities, synopses carrying the precise errors discussed in this article are routinely submitted, reviewed, and registered for study. A title that says “An open-label randomised controlled trial to evaluate the efficacy of Formulation X as compared to the standard drug Formulation Y in the management of Condition Z” — where Formulation Y was studied in a 30-patient open-label dissertation six years ago, where the randomisation is actually alternating allocation, where there is no allocation concealment, no independent outcome assessor, and no a priori sample size calculation — passes through the synopsis committee without comment and receives university registration.
This is not speculation. Any person who has attended a synopsis presentation committee in an Ayurvedic institution in the last decade has witnessed it. The errors are not subtle. They are visible to anyone with a working knowledge of clinical research methodology. They pass because the people in the room do not have that knowledge — or because institutional culture has normalised the errors to the point where raising them feels disruptive rather than obligatory.
Dissertations Are Approved on the Same Flawed Foundations
The study is then conducted — with the same design flaws embedded in the registered synopsis, because the scholar has no structural reason to correct what the institution already approved. The dissertation is submitted. An external examiner is appointed. The viva voce is conducted. In the overwhelming majority of cases, the dissertation is approved — with minor corrections at most, none of which address the fundamental methodological problems that were present from the title stage.
What does this approval signify? Formally, it signifies that the research meets the standards of the awarding university for the degree of MD (Ayu) or PhD. Functionally, it signifies something far more troubling: that the guide who supervised the work, the internal examiner who reviewed it, the external examiner who evaluated it, and the university that awarded the degree all either did not identify the methodological errors or did not consider them disqualifying. In either case, the credential — the MD, the PhD — has been awarded for work that would not survive scrutiny by any competent clinical research methodologist.
This is a credential problem of the first order. A degree is an institutional claim about the competence of its holder. When that degree is awarded on the basis of methodologically indefensible research, the claim is false. The degree holder is not necessarily incompetent — they were trained within a system that did not demand competence in research methodology. But the credential implies a standard that was never applied.
The Guide and Examiner as the Weakest Links
It is important to be direct about where the primary responsibility lies, because diffuse institutional blame has a way of absolving everyone.
The guide is the scholar’s primary intellectual supervisor. The guide is responsible for ensuring that the research question is original, that the study design is appropriate to the question, that the sample size is justified, that the comparator is legitimate, and that the title accurately represents the study. When a guide approves a synopsis with a title that claims an RCT where none exists, or a standard comparator that was never validated, the guide has failed in the most fundamental supervisory obligation. The fact that this failure is widespread does not make it less serious. It makes it systemic.
The examiner — internal and external — is the final methodological checkpoint before the university awards the degree. An examiner who does not scrutinise study design, does not ask how randomisation was achieved, does not ask what justified the sample size, does not ask what evidence established the comparator as a standard, and does not ask what the confidence intervals around the effect estimate are — is not performing the examiner’s function. The viva voce in Ayurvedic PG and PhD programmes has, in too many institutions, become a ceremonial event rather than a methodological interrogation. This must change.
The examiner who lacks the knowledge to ask these questions should not be examining research dissertations. The guide who lacks the knowledge to catch these errors should not be guiding research scholars. These are not harsh judgments — they are the minimum expectations of a credentialing system that takes its own credentials seriously.
The Publication Pipeline: From Flawed Dissertation to Predatory Journal
The institutional failure does not end at the degree. Most Ayurvedic universities and regulatory bodies now require PG and PhD scholars to publish their research — in a journal, before or shortly after dissertation submission — as a condition of degree completion or as evidence of scholarly productivity. This requirement, well-intentioned in principle, has in practice created a direct pipeline from methodologically flawed dissertation research to published literature. And the journals receiving this research are, in a large and growing proportion of cases, predatory.
Predatory journals — those that charge article processing fees, conduct no genuine peer review, publish within days or weeks of submission, carry no legitimate indexing, and exist primarily as revenue-generating vehicles for their operators — have found a captive market in Ayurvedic PG and PhD scholars who need a publication to satisfy their university requirement and whose institutions do not scrutinise where that publication appears. The scholar pays the fee. The journal publishes the article, typically without requesting revisions, within a timeframe that makes genuine review structurally impossible. The publication requirement is satisfied. The degree is awarded.
What has been accomplished? The flawed research — with its mislabelled design, its 30-patient sample, its cascading comparator, its open-label convenience allocation masquerading as randomisation — now exists in the published literature. It has an ISSN. It has a DOI. It is citable. And it will be cited — by the next generation of PG scholars constructing the evidence base for their own comparators, extending the self-referential evidence loop discussed earlier and adding another layer of pseudovalidation to a claim that was never validated in the first place.
This is how flawed research compounds. Not through malice, but through a system that has no functional quality control at any stage — from title to synopsis committee, from committee to guide approval, from guide approval to university registration, from registration to dissertation, from dissertation to examiner, from examiner to degree, from degree to publication, from publication to the next scholar’s literature review.
What This Means for Ayurveda’s Epistemic Standing
The consequences are not merely internal to the institutions that produce this research. They extend to every context in which Ayurvedic research is presented as evidence — to regulatory bodies, to policy makers, to international academic collaborators, to biomedical researchers evaluating whether Ayurvedic claims merit serious investigation, and to patients and practitioners who rely on published research to make treatment decisions.
When a systematic review of Ayurvedic interventions for a given condition draws on the published literature and finds that the evidence base consists predominantly of small, open-label, single-institution studies published in non-indexed journals with methodological weaknesses that were never flagged by peer review, the conclusion is predictable: the evidence is insufficient to support clinical recommendations. This conclusion is correct. But it is interpreted, often, as evidence that Ayurvedic interventions lack efficacy — when what it actually evidences is that Ayurvedic research lacks methodological rigour. These are not the same statement. The first is a claim about the knowledge system. The second is a claim about the institutions that are failing to produce credible evidence for it.
Ayurveda as a knowledge system is not diminished by the failures of its research institutions. But it is being misrepresented by them. And that misrepresentation has a cost — in credibility, in policy influence, in international academic standing, and in the long-term sustainability of a tradition that deserves far better than the evidence base currently being built in its name.
The scholars, guides, examiners, journal editors, and university administrators who perpetuate this system are not, in the main, acting in bad faith. They are acting within the norms of an ecosystem that was never designed for the level of methodological rigour that contemporary research standards demand. But ignorance of a problem does not constitute immunity from its consequences. And at this point, the problems are sufficiently well documented — in AYUSH ministry reports, in academic critiques, in the commentaries of international reviewers — that continued ignorance is difficult to distinguish from indifference.
Reform begins with the title. It begins with a guide who refuses to approve a synopsis that does not answer to PICO. It begins with an examiner who asks, in the viva, exactly how the randomisation was performed. It begins with a scholar who understands that calling a study an RCT when it is not one is not a technicality — it is a misrepresentation of knowledge. And it begins with an institution that measures its research credibility not by the number of dissertations registered and publications submitted, but by the methodological quality of the evidence it produces.
That is the standard Ayurveda deserves. It is time the institutions that claim to advance it began to hold themselves to it.
Summary: The Title Checklist
Before submitting your synopsis title, verify it against this checklist:
- P — Is the population/problem defined with specificity (age, gender, diagnosis with classical and contemporary labels, severity or stage)?
- I — Is the intervention named precisely (formulation, route, dosage context, classical source where applicable)?
- C — Is the comparison/control stated or clearly implied?
- O — Is at least one measurable outcome specified or strongly implied?
- T — Is the time frame stated where it is clinically or methodologically important?
- Have you conducted a genuine literature search that demonstrates this study is original and needed?
- Does your title pass the relevance test — prevalent condition, available intervention, appropriate outcome, ethical feasibility?
- Is the title free of vague action words like “role of,” “effect of” without specifying the direction, or “comparative study” without naming what is being compared?
- Does it use dual nomenclature correctly — Ayurvedic and contemporary — without false equivalence?
- Is it a single, clear, defensible sentence?
If the answer to any of these is No, your title is not yet ready.
Closing Thought
The title of your research synopsis is not the first thing you write. It is the last. It is the crystallisation of your understanding of the subject, the literature, the clinical context, and the methodological constraints of your study. When written in haste, it betrays that haste immediately. When written with rigour, it announces your credibility as a scholar before the committee reads another line.
Ayurvedic research is at an inflection point. The field needs scholars who do not just fill the traditional roles of the Vaidya but who can also speak the language of evidence with authority, precision, and intellectual honesty. The title of your synopsis is where that conversation begins. Make it count.
This article is part of the Ayurveda Unfiltered series — critical scholarship for a field that deserves better than comfortable silence.
Share your thoughts in the comments below.
💬 Comments & Discussion